- Original Research Article
- Open access
- Published:
Phencyclidine false positive induced by lamotrigine (Lamictal®) on a rapid urine toxicology screen
International Journal of Emergency Medicine volume 3, pages 327–331 (2010)
Abstract
Background
This report describes two cases with unexplained positive results for phencyclidine (PCP).
Aims
This case will correlate lamotrigine (Lamictal®) use with false-positive results for PCP on a rapid urine toxicology screen.
Methods
Case 1: A 62-year-old male arrived to the emergency department in extreme psychosis. All positive results on the urine drug screen could be accounted for except PCP. A comprehensive drug screen was performed to confirm PCP use, but returned negative. PCP was ruled out as the causative agent. The reason for the PCP false positive remained unknown. Case 2: A 49-year-old female presented to the ED with a history of seizures and depression. Despite positive PCP results on a rapid urine drug screen, PCP use was ruled out due to patient presentation and comprehensive history.
Results
The differential diagnosis in case 1 included PCP abuse until PCP was ruled out by a comprehensive drug screen. A literature search failed to explain a reason for false-positive results. The patient in case 2 was not psychotic, but returned a positive urinalysis result for PCP. Case 2’s presentation combined with a comprehensive history at the facility ruled out PCP use. Both patients were taking the anti-seizure medication lamotrigine with nothing else in common.
Conclusion
Lamotrigine has the potential to cause false-positive results for PCP on the Bio-Rad TOX/See urine toxicology screen.
Introduction
Modern rapid urine drug testing kits sometimes provide false-positive results that may cloud clinical pictures. This report describes two patients presenting to the emergency department (ED) with unexplained positive results for phencyclidine (PCP) on a rapid urine toxicology screen.
Background
-
Case 1
A psychotic 62-year-old male arrived to the ED extremely agitated with violent behavior. The patient’s wife described a history of narcotic abuse, violent behavior, self harm, and lighting fires in the house and yard. She expressed extreme worry and feared for both their safety. The patient was uncooperative, delirious, and required sedation and soft restraints to prevent injury to himself and staff.
The patient was examined by the ED physician and found to be in good physical health with no obvious trauma. The patient had no prior history at the facility, and medical records were unavailable. Vital signs were stable, and CBC and Chem-7 were unremarkable, with the exception of a high blood glucose at 244 mg/dl. A rapid urine drugs of abuse (DOA) screen (Bio-Rad TOX/See test kit) returned positive results for methadone, oxycodone and PCP. Methadone and oxycodone were both part of the patient’s home medication regimen (see Fig. 1). The patient was unable to reliably state what medications he had ingested recently and whether or not he used recreational drugs. The patient’s home medication bottles were brought by the wife to the ED. Investigation revealed that pill counts corresponded with latest medication fill, likely indicating proper use and ruling out an apparent intentional overdose using prescription medications. Positive results on the urine DOA for oxycodone and methadone were expected. Negative results for benzodiazepines could possibly be explained by an “as needed” use of the medications and/or the fact that some urine tests have an inability to detect clonazepam [1]. The positive PCP result was unexpected.
Fig. 1 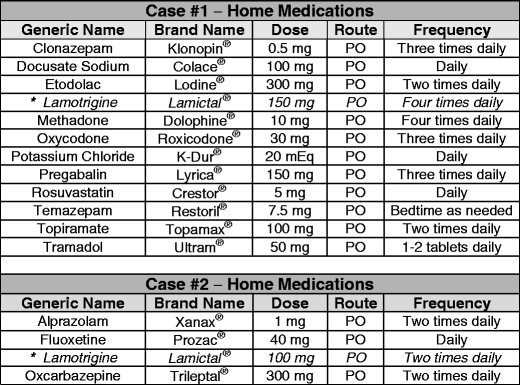
Patient home medications
Patient age and current local usage trends argued against PCP intoxication, whereas the history of drug abuse, violent behavior and delusions justified sending a urine sample for a comprehensive drug screen. Contrasting with the rapid urine DOA screen, the colorimetric comprehensive screen detected benzodiazepines, methadone, oxycodone and oxymorphone. PCP was not detected. The reason for the PCP false positive remained unknown. Patient records were eventually located at another institution and revealed a history of mental instability. PCP was ruled out as a causative agent.
-
Case 2
Weeks later, a 49-year-old female was transported to the ED by ambulance. The patient had a history of bipolar and depressive disorders as well as a history of seizures. As the patient arrived on a stretcher, she was somnolent but in no acute distress. She was examined by the ED physician and found to be in good general health with no pain or obvious trauma. The patient’s mother stated that her daughter said her tongue felt swollen then she became stiff and fell to the floor. Upon initial examination, the patient had a blunt affect and some rigidity in her extremities; she also felt nauseous. CBC and Chem-7 were unremarkable. A rapid urine DOA screen (Bio-Rad TOX/See test kit) revealed positive results for benzodiazepines and PCP. The positive result for benzodiazepines was expected as the patient was taking alprazolam; the positive result for PCP was unexpected.
As the patient became more aware, she reported having felt disorientated for 2 days prior and experienced involuntary jerking and seizure-like activity that morning. She stated that she is adherent to her prescribed medication regimen and that she does not abuse recreational drugs or prescription medications. The patient manages her therapy through out-patient psychiatry visits and prescription medications (see Fig. 1). A serum lamotrigine level was sent to document use and resulted in a value of 7.6 mcg/ml (reference range 0.25-29.1 mcg/ml) [2]. Recently the patient had been prescribed a new medication, oxcarbazepine (Trileptal®), to assist in controlling her seizure disorder. She did not use any herbal remedies and had no recent use of over-the-counter products. The patient had a consistent history of treatment at the facility, and the use of PCP by this patient was ruled out. Likely, this patient suffered from breakthrough seizure or an episode of tardive dyskinesia because of the addition of the new medication. The patient was discharged home the same day with instructions to follow-up with her neurologist.

Discussion
PCP was developed in the 1950s as an intravenous anesthetic. Its use was discontinued due to dramatic and intense side effects, including hallucinations, delusions, anxiety and agitation. PCP has no current medical use, but is sold illicitly in multiple forms. Under the influence of PCP, users hallucinate and exhibit rapid, intense emotional swings. Abusers can experience unpleasant psychological effects with symptoms mimicking schizophrenia (delusions, hallucinations, disordered thinking, extreme anxiety) [3]. Yago et al. reported that 50% of individuals brought to the ED because of PCP use have significant anxiety combined with a variety of psychotic clinical symptoms bordering on mania, depression and/or schizophrenia [4]. PCP can be seen in the urine 4-6 h after use and can be detected for up to 14 days [5].
A current rise in PCP abuse combined with violent crime has made recent headlines in Washington, DC. Police report that violent crimes involving PCP use have increased 9% from 2007. Drug addicts appear to be looking for a longer lasting high. A crack cocaine high lasts only minutes; PCPs effects can last from 3-6 h [6]. The Monitoring the Future Survey conducted annually by the University of Michigan’s Institute for Social Research found that in 2007, 6.1 million persons aged 12 or older have used PCP. In 2008, 1.8% of high school seniors admitted using PCP in their lifetime, while past-year use was reported at 1.1% [7].
The advent of rapid urine screening tests for drugs of abuse has provided the clinician with access to quick information regarding a battery of potential drugs of abuse that patients might have had exposure to, ingested, inhaled or used intravenously. Rapid screen kits are calibrated and have cut off concentrations as decided by the Department of Health and Human Services (DHHS) Substance Abuse Mental Health Services Administration (SAMSHA) [8–10]. Bio-Rad’s TOX/See test kit is a urine-based, lateral flow chromatographic immunoassay. It is a one-step, hand-held, point-of-care test device for the qualitative detection of 14 drugs and their metabolites in human urine. The TOX/See guide states results are available in 5 min after application of urine to the test kit, with results remaining stable for up to 1 h afterwards [5].
The patient in case 1 presented to the ED in psychotic duress. Urine was collected via straight catheterization. The Bio-Rad Laboratories TOX/See rapid urine test was used and returned the positive result for PCP. The comprehensive drug screen returned negative for PCP and overturned the hypothesis that the psychosis was related to PCP use. The Bio-Rad Tox/See package insert was consulted and made no mention of possible cross reactants with phencyclidine [5]. A literature search was conducted to see if any of the home medications might cause a false positive. Searches were conducted using PubMed and various combinations of search terms: “phencyclidine,” “PCP,” “false,” “positive,” “urine” and “test.” Also included was a search on false positives reported on all generic and brand names of home medications the patient was reportedly ingesting. Results showed six case reports documenting venlafaxine (Effexor®, Wyeth) and dextromethorphan (DM) as known agents that cause false positives for PCP on rapid urine drug tests [11–17]. The patient was not on venlafaxine, and according to the Bio-Rad package insert, DM does not cross react at a concentration of 100 mcg/m-, so an over-the-counter overdose of DM could be eliminated (although DM is known to cross react in 4 of 8 commonly marketed kits) [1, 5].
A single case report with chloroquine and one postmortem tramadol (Ultram®) urine specimen showed false positives for PCP [18, 19]. This patient was not known to be on chloroquine but was taking tramadol at home. Hull and colleagues reported a false positive for PCP involved in a fatal single-drug overdose involving tramadol. They measured a serum tramadol level of 14 mg/l, orders of magnitude above therapeutic ranges and the highest tramadol level reported at the time of the case [19]. Their experiment demonstrated that the false positive for PCP was due to the extremely high level of tramadol. Further, they showed that lower levels of the medication resulted in cutoff values below positive results for PCP on their test, demonstrating the false positive in that case was due to their specific immunoassay combined with the extremely high level of tramadol. In the present case, there was no evidence of intentional or accidental overdose with tramadol, as the pill counts corresponded with the medication fill date and prescription instructions on the pill bottle. Our patient was not sedated and did not suffer from any drug-induced respiratory depression. Tramadol was not suspected as a causative agent for the psychosis, and a serum tramadol level was not obtained.
As a thorough literature search and the test kit package insert failed to provide possibilities for the positive PCP result, Bio-Rad technical support was contacted. Our query was elevated to a specialist who later provided a copy of the Bio-Rad TOX/See Cross Reactivity Guide. The unpublished guide lists venlafaxine as a “potential” cross reactant and lamotrigine (Lamictal®, GlaxoSmithKline) as the only known medication to cause false-positive results for PCP on their rapid urine screen [20]. Bio-Rad’s guide is a manufacturer document and does not reference any specific cases, measured cutoff values for the drugs, or any scientific data on why or how these cross react. There are multiple published case reports in the literature describing venlafaxine-induced false positives for PCP; there are none for lamotrigine.
The patient in case 2 presented to the ED via ambulance and was arousable upon arrival. She was not altered, psychotic or under duress. Blood and urine samples were provided willingly by the patient. The Bio-Rad Laboratories TOX/See point-of-care rapid urine test was used to assess potential DOA and the positive benzodiazepine and PCP results returned shortly thereafter. Based on current symptoms and history at the facility, recreational PCP abuse was not considered as a differential diagnosis. The patient provided a logical sequence of events and denied use of any illicit drugs, over-the-counter medications and/or herbal remedies. A literature search was conducted on all generic and brand names of her prescriptions. None were implicated in providing false-positive results on any DOA screen. The patient was taking her prescribed lamotrigine as verified by a serum level of 7.6 mcg/ml. Due to the patient presentation, comprehensive history at the facility, current PCP usage trends and information provided by Bio-Rad’s cross-reactivity guide, PCP use was ruled out, and the false-positive result was blamed on lamotrigine.
Results
Lamotrigine is the common bond that links these two cases with regards to the false-positive results for PCP. During case 1 the patient was actively psychotic, and recreational drug use needed to be ruled out through the comprehensive drug screen. No previous documentation in the literature was able to explain the false positive for PCP until the manufacturer was contacted. Case 2 provided evidence that illicit drug use was not involved with the positive result, and a lamotrigine serum level established that the patient was compliant with her home medications.
Conclusion
Lamotrigine has the potential to provide a false-positive result for PCP on the Bio-Rad TOX/See rapid urine toxicology screen. Aside from the unpublished Bio-Rad cross-reactant list, which is available from the company technical support division on request, this is the first known report published in the medical literature that describes this cross reaction. Clinicians wishing to rule out PCP-induced psychosis should be aware of this potentially confounding result. The clinical symptoms of delirium, agitation and psychosis may not be attributable to PCP if the patient is taking lamotrigine. Further research is warranted to elucidate the basis for the false-positive PCP result caused by lamotrigine on this and other rapid urine DOA assays.
References
Krasowski M, Pizon A, Siam M et al (2009) Using molecular similarity to highlight the challenges of routine immunoassay-based drug of abuse/toxicology screening in emergency medicine. BMC Emerg Med 9(1):5
Lacy C, Armstrong L, Goldman M et al (eds) (2008) Lexi-comp drug database drug information handbook, 17th edn. Lexi-Comp Information Management Service (LIMS), Hudson, OH, pp 885–887
Jacob MS, Carlen PL, Marshman JA et al (1981) Phencyclidine ingestion: drug abuse and psychosis. Int J Addict 16(4):749–758
Yago KB, Pitts FN Jr, Burgoyne RW et al (1981) The urban epidemic of phencyclidine (PCP) use: Clinical and laboratory evidence from a public psychiatric hospital emergency service. J Clin Psychiatry 42(5):193–196
Bio-Rad Laboratories (2009) TOX/See drug screen test package insert. Number: 1155895805
Alexander KL (2009) “Scary Drug” Makes Comeback—As PCP Use Rebounds Among Suspects, DC. Authorities Worry About Violent Incidents. Washington Post. (http://www.washingtonpost.com/wp-dyn/content/article/2009/03/16/AR2009031603178.html) Accessed: 2/9/2010, Published: 3/17/2009
Johnston LD, O’Malley PM, Bachman JG et al. Monitoring the future, national results on adolescent drug use: Overview of key findings, 2008. The University of Michigan Institute for Social Research 2009;NIH Publication No. 09-7401 (http://www.monitoringthefuture.org/) Accessed: 2/9/2010
Moeller KE, Lee KC, Kissack JC (2008) Urine drug screening: practical guide for clinicians. Mayo Clin Proc 83(1):66–76
Department of Health and Human Services (DHHS) Substance Abuse Mental Health Services Administration (SAMSHA) http://workplace.samhsa.gov/DrugTesting/RegGuidance/UrineConcen.aspx. Accessed: 2/9/2010
Vogl WF (2004) Federal Register: Mandatory Guidelines and Proposed Revisions to Mandatory Guidelines for Federal Workplace Drug Testing Programs; Notices. DHHS - SAMSHA. 69(71)
Santos PM, Lopez-Garcia P, Navarro JS et al (2007) False positive phencyclidine results caused by venlafaxine. Am J Psychiatry 164(2):349
Schier J, Díaz JE (2000) Avoid unfavorable consequences: dextromethorphan can bring about a false-positive phencyclidine urine drug screen. J Emerg Med 18(3):379–381
Schwartz RH (2005) Adolescent abuse of dextromethorphan. Clin Pediatr 44(7):565–568
Sena SF, Kazimi S, Wu AHB (2002) False-positive phencyclidine immunoassay results caused by venlafaxine and O-desmethylvenlafaxine. Clin Chem 48(4):676–677
Bond GR, Steele PE, Uges DRA (2003) Massive venlafaxine overdose resulted in a false positive abbott AxSYMA urine immunoassay for phencyclidine. Clin Toxicol 41(7):999–1002
Budai B, Iskandar H (2002) Dextromethorphan can produce false positive phencyclidine testing with HPLC. Am J Emerg Med 20(1):61–62
Romanelli F, Smith KM (2009) Dextromethorphan abuse: clinical effects and management. J Am Pharm Assoc (2003) 49(2):20–25
Collins GB, McAllister MS (2008) Chloroquine psychosis masquerading as PCP: a case report. J Psychoactive Drugs 40(2):211–214
Hull M, Griggs D, Knoepp S et al (2006) Postmortem urine immunoassay showing false-positive phencyclidine reactivity in a case of fatal tramadol overdose. Am J Forensic Med Pathol 27(4):359–362
Bio-Rad Laboratories (2007) TOX/See urine drug screen tests technical information—troubleshooting guide crossreactivity tables. 18
Acknowledgements
The authors would like to acknowledge Michael Orris, DO, and Elliot Blum for their assistance.
Conflicts of interest
None.
Author information
Authors and Affiliations
Corresponding author
Additional information
The views expressed in this paper are those of the author(s) and not those of the editors, editorial board or publisher.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 2.0 International License (https://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
About this article
Cite this article
Geraci, M.J., Peele, J., McCoy, S.L. et al. Phencyclidine false positive induced by lamotrigine (Lamictal®) on a rapid urine toxicology screen. Int J Emerg Med 3, 327–331 (2010). https://doi.org/10.1007/s12245-010-0235-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12245-010-0235-3