- Review
- Open access
- Published:
Bradykinin-induced angioedema in the emergency department
International Journal of Emergency Medicine volume 15, Article number: 15 (2022)
Abstract
Background
Acute airway angioedema commonly occurs through two distinct mechanisms: histamine- and bradykinin-dependent. Although they respond to distinct treatments, these two potentially life-threatening states present similarly. Poor recognition of the bradykinin-dependent pathway leads to treatment errors in the emergency department (ED), despite the availability of multiple pharmacologic options for hereditary angioedema (HAE) and other forms of bradykinin-induced angioedema. Here, we consider the pathophysiology and clinical features of bradykinin-induced angioedema, and we present a systematic literature review exploring the effectiveness of the available therapies for managing such cases.
Methods
PubMed searches using ‘emergency’, ‘bradykinin’ and various therapeutic product names identified studies reporting the efficacy of treatments for bradykinin-induced angioedema in the ED setting. In all, 22 studies met prespecified criteria and are analysed here.
Findings
Whereas histamine-induced angioedema has a faster onset and often presents with urticaria, bradykinin-induced angioedema is slower in onset, with greater incidence of abdominal symptoms. Acute airway angioedema in the ED should initially be treated with anaphylactic protocols, focusing on airway management and treatment with epinephrine, antihistamine and systemic steroids. Bradykinin-induced angioedema should be considered if this standard treatment is not effective, despite proper dosing and regard of beta-adrenergic blockade. Therapeutics currently approved for HAE appear as promising options for this and other forms of bradykinin-induced angioedema encountered in the ED.
Conclusion
Diagnostic algorithms of bradykinin-induced angioedema should be followed in the ED, with early use of approved therapies to improve patient outcomes.
Background
Obstruction of the upper airway due to angioedema is a life-threatening event. Most such attacks are caused by an allergic reaction mediated by histamine. However, a non-allergic form mediated by bradykinin is also seen and may be mistaken for histamine-induced angioedema.
Because these types of angioedema respond to distinct treatments, prompt diagnosis is essential for reversing a potentially fatal airway attack. This article presents a clinical algorithm adapted from evidence-based guidelines, addressing the management of bradykinin-induced angioedema in the ED, as well as a systematic literature analysis examining the treatment of bradykinin-induced angioedema in the ED setting.
Methods
A systematic literature search in PubMed was conducted to identify articles addressing bradykinin-induced angioedema treatment in the ED setting, using the search terms ‘plasma-derived C1-INH’ or ‘recombinant C1-INH’ or ‘ecallantide’ or ‘icatibant’ or ‘fresh frozen plasma’ and ‘emergency’ and ‘bradykinin’. Of 137 prospective and retrospective studies, case series and case reports identified, 122 were excluded because they did not describe ED treatment of bradykinin-induced events or did not report treatment efficacy. Seven additional studies were identified by targeted searches or scanning bibliographies, for a total of 22 studies analysed below.
What is the pathophysiology of bradykinin-induced angioedema and how does it differ from histamine-induced angioedema?
Angioedema is characterised by the localised increase of vascular permeability and dilation, triggered by the release of mediators such as histamine or bradykinin [1,2,3,4,5]. The mechanism underlying histamine-induced (allergic) angioedema is shown in Fig. 1A [2, 6, 7]. During first exposure to an allergen, specific immunoglobulin E (IgE) antibodies sensitise mast cells by binding high-affinity IgE receptors (FcεRI). During a re-encounter, allergen binding to IgE-FcεRI complexes promotes release of histamine, which binds receptors on the vascular endothelium, triggering angioedema.
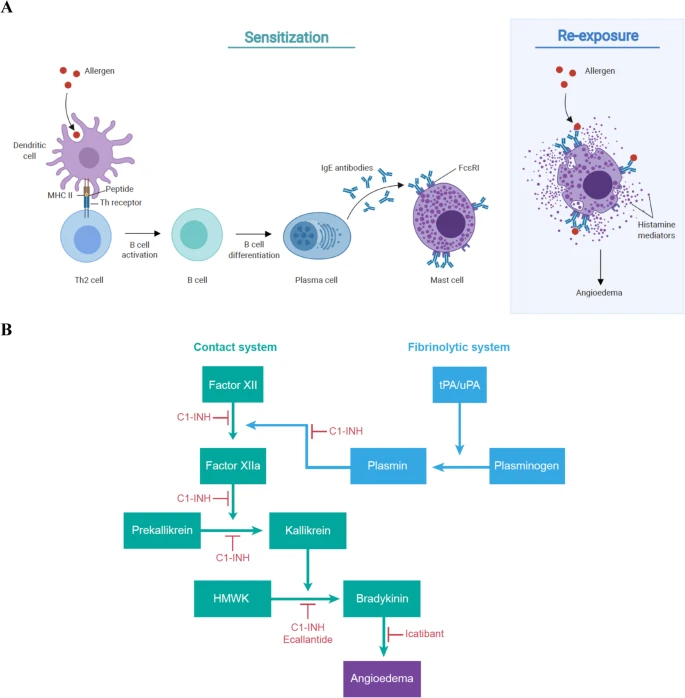
Mechanisms of angioedema [2, 6,7,8]. A Histamine induced. Upon exposure to an allergen, it is taken up by antigen-presenting cells (e.g. dendritic cells) and proteolyzed to produce small peptides. These peptides are then presented with major histocompatibility (MHC) class II antigen as a complex on the cell surface and recognised by T-helper (Th) lymphocyte receptors. This leads to the activation of T cells and release of Th2 cytokines that promote the differentiation of B cells to plasma cells and the production of specific IgE antibodies that recognise the original antigen. These antibodies bind to high-affinity IgE receptor FcεRI on mast cells and persist for weeks, months or years. Upon re-exposure to the allergen, the allergenic peptide is recognised by these bound IgEs, activating the mast cells to release bioactive mediators such as histamine. Binding of histamine on selective receptors of the vascular endothelium causes vasodilation and increased permeability. Mast cells can also be activated and triggered to produce histamine mediators through non-IgE-mediated response. B Bradykinin-induced. The contact pathway is initiated when factor XII (or Hageman factor) binds to damaged tissue and converts to factor XIIa, which then converts prekallikrein to plasma kallikrein. Finally, kallikrein cleaves HMWK to form bradykinin, which binds B2 receptors on the vascular endothelium, triggering vasodilation and increased permeability. Plasmin from the fibrinolytic system can convert factor XII into factor XIIa, accelerating the bradykinin production from HMWK. Multiple biological and pharmacological inhibitors can be used to treat bradykinin-induced angioedema. C1-INH can act on multiple stages of the contact and fibrinolytic system to inhibit the production of bradykinin. Ecallantide is a kallikrein inhibitor that blocks the cleavage of HMWK into bradykinin, and icatibant is an antagonist that prevents bradykinin from binding to its receptor
Bradykinin-induced angioedema may be hereditary, acquired or drug induced [1, 2, 4, 5]. Bradykinin is generated through the cleavage of high-molecular-weight kininogen (HMWK) by activated kallikrein as shown in Fig. 1B [2, 8]. Kallikrein activation occurs through the contact system via factor XII, which can be activated by plasmin through the fibrinolysis pathway. Bradykinin binds the bradykinin B2 receptor on the vascular endothelium, stimulating substance P release and inducing angioedema.
C1 esterase inhibitor (C1-INH), which acts as a brake on the complement system, blocks bradykinin overproduction via the contact system. Hereditary angioedema (HAE) arises from mutations in the gene encoding C1-INH, reducing its expression (type I) or function (type II) [1, 2, 4, 5, 9]. Nonhereditary angioedema is caused by C1-INH overconsumption, which can occur with lymphoproliferative or autoimmune disease. In drug-induced angioedema, bradykinin or substance P turnover is blocked due to inhibition of catabolic enzymes including angiotensin-converting enzyme (ACE), neprilysin, dipeptidyl peptidase 4, carboxypeptidase and aminopeptidase P [10].
What are key clinical features that differentiate bradykinin-induced angioedema from histamine-induced angioedema?
Although there are no validated tests available to quickly distinguish between histamine- or bradykinin-induced angioedema in the ED setting, differences in the typical clinical presentation of these distinct conditions (Table 1) can help guide diagnosis [1, 2, 4, 5].
Histamine-induced angioedema often presents with urticaria and other manifestations of anaphylaxis such as bronchospasm, wheezing and hypotension. Onset is rapid and attack duration may be brief. In contrast, bradykinin-induced angioedema is usually not associated with urticaria and tends to have slower onset, longer duration and involve abdominal symptoms. A defining feature that distinguishes between these two types of angioedema is that bradykinin-induced angioedema responds poorly, if at all, to epinephrine, antihistamines or corticosteroids [1,2,3,4,5].
What is the current approach to identify and manage bradykinin-induced angioedema in the ED?
Consistent with existing guidelines [1, 3,4,5], the algorithm in Fig. 2 shows the first priority for any patient presenting with angioedema in the ED is assessment of obstruction in the upper airway. All patients with head, neck or lingual angioedema may benefit from flexible fiberoptic nasopharyngolaryngoscopy to determine the extent of swelling. Attempted awake intubation should proceed with an ‘airway double setup’, wherein equipment and bedside expertise are available to initiate emergency tracheotomy or cricothyrotomy if needed [5]. If a pre-existing diagnosis of HAE is known, an appropriate treatment, such as C1-INH may be administered at this point [1,2,3,4,5].

ED response to localised airway angioedema, consistent with published algorithms [1, 3, 4]. When a patient presents at the ED with localised angioedema, airway management should be performed and intubation, tracheotomy or cricothyrotomy procedures should be prepared for worsening symptoms. Unless the patient is known to have HAE or reports prior experience of ACEi- or similar drug-induced angioedema, it is usually difficult to differentiate between histamine- or bradykinin-induced angioedema by clinical presentation alone. Because histamine-induced angioedema is more common, the patient should receive standard treatment (epinephrine, antihistamine and/or corticosteroids). If the symptoms subside, this helps confirm the aetiology as histamine-induced angioedema. Conversely, if symptoms do not resolve or begin to worsen, and beta-adrenergic blockade has been excluded, bradykinin-induced angioedema becomes more likely. Although approved treatments are currently for HAE, some studies have reported that patients with suspected bradykinin-induced angioedema in the ED respond well to these treatments. However, more studies are required to establish their efficacy and use in emergency situations. The patient’s primary care physician should be notified, and the patient should be referred to a specialist if appropriate for long-term management
When the underlying cause of angioedema is unknown, standard treatment with epinephrine, antihistamines or corticosteroids should be administered [1, 3, 4]. In the case of a satisfactory response, diagnosis of histamine-induced angioedema is supported, and the patient may be referred to a specialist for long-term management and counselling on the use of an epinephrine autoinjector [1,2,3, 5]. In the case of non-optimal response, beta-adrenergic blockade should be considered [11]. Otherwise, the index of suspicion rises for a bradykinin-induced aetiology, especially if the patient is on ACE inhibitors (ACEis). Following resolution of a bradykinin-induced episode, patients’ primary care physician should be contacted to discuss medication changes or specialist care, which may be appropriate to confirm the diagnosis supported by laboratory investigation and for long-term management of patients with HAE [1,2,3].
How can bradykinin-induced angioedema be treated in the ED?
Table 2 outlines therapeutic options available for HAE in the USA. These treatments are less well studied in acquired- or drug-induced angioedema. Three C1-INH concentrate products are available to inhibit bradykinin biogenesis, as shown in Fig. 1B: plasma-derived C1-INH (Berinert) is approved for treating acute abdominal, facial or laryngeal HAE attacks in adults and paediatric patients; plasma-derived C1-INH (Cinryze) is approved for the routine prophylaxis against angioedema attacks in adults, adolescents and paediatric patients ≥6 years with HAE; and recombinant C1-INH (conestat alfa) is approved for acute attacks in adults and adolescents patients with HAE [12,13,14,15,16,17]. Icatibant (Firazyr) is a synthetic selective bradykinin receptor antagonist that is approved for acute attacks of HAE in adults, and ecallantide (Kalbitor) is a kallikrein inhibitor that is approved for acute attacks of HAE in patients ≥12 years [18,19,20,21]. Although these treatments are approved in the USA, they may not be approved in all other countries. For example, conestat alfa and ecallantide are not licensed in Canada, but may be accessed through Health Canada’s Special Access Programme [22,23,24]. In situations when these agents are not available, fresh frozen plasma (FFP) containing C1-INH should be considered as an alternative treatment option for HAE attacks [25,26,27].
How effective are the available treatments for bradykinin-induced angioedema in resolving acute attacks in the ED?
Of 22 studies describing the treatment of bradykinin-induced events in the ED (Fig. 3), eight focused on CI-INH, eight on icatibant, one on CI-INH or icatibant, two on ecallantide and three on FFP. These studies include eight prospective studies, one retrospective study, six case series and seven case reports. Most describe drug-induced attacks (16/22); the remainder describe emergency management of HAE attacks. No reports on acquired angioedema were identified. No unexpected safety signals emerged for any of the products studied in these papers.

Consort diagram of systematic literature search. Search terms on PubMed generated a total of 137 studies. Those that were not conducted in the ED setting, related to treatment efficacy and/or bradykinin-induced angioedema were excluded (n = 122). Seven additional papers relevant to the discussion of the review were included in the analysis. The final 22 studies reported on the effectiveness of current treatments for resolving acute bradykinin-induced angioedema attacks in the ED
HAE
In a prospective study of 95 patients, 193 emergency laryngeal edema episodes in 42 HAE patients were treated with C1-INH concentrate [30]. The mean episode duration declined 85% with C1-INH (15.3 ± 9.3 h) compared with historical attacks in the same patient population when C1-INH was not used (100.8 ± 26.2 h). Shorter median time to symptom resolution (8.25 h) was also observed in a prospective study with 16 patients treated with C1-INH who experienced 39 emergency laryngeal attacks [31]. Similarly, in two case studies of emergency HAE attacks (one with previously undiagnosed HAE), symptom resolution occurred with C1-INH, whereas standard therapy showed no response [32, 33]. In a retrospective study of 176 emergency episodes amongst 43 patients, 96/98 episodes resolved within 4 h of FFP treatment (IQR: 2–12) [34]. Symptom resolution was also observed amongst three patients treated with FFP in a case series of emergency HAE episodes [35]. These studies demonstrate that C1-INH and FFP are effective in treating HAE attacks in an ED setting.
Drug-induced angioedema
Three case reports and one case series describe a total of 14 patients with suspected ACEi-induced angioedema treated in the ED with C1-INH [36,37,38,39]. Symptoms resolved in 13 patients. One patient, who experienced a relapse 4 h after treatment, underwent tracheotomy [38]. None of the 10 patients treated with C1-INH from the same case series required intubation or tracheotomy compared to the historical control group who received standard treatment at the same institution (3/47, 6.38% required tracheotomy; 5/47, 10.64% required intubation) [37]. These reports support the idea that C1-INH is effective in treating drug-induced angioedema and that it may avoid the need for invasive interventions.
Studies assessing ED use of icatibant for ACEi-induced angioedema are inconsistent. In two case reports and three case series describing 36 patients with suspected ACEi-induced angioedema, all patients experienced clinical improvement, with symptom regression time of 0.5–7 h following icatibant treatment [40,41,42,43,44]. In a prospective study of 62 patients across EDs of four hospitals, patients were provided with C1-INH, icatibant or standard treatment [45]. C1-INH or icatibant led to significantly shorter time to symptom relief relative to standard treatment (0.5 h [IQR: 0.5–1.0] C1-INH or icatibant versus 3.9 h [IQR: 2.5–7.0] standard treatment, p < 0.0001). In a phase 2 randomised controlled trial (RCT) of 27 patients, complete symptom resolution occurred more quickly with icatibant (8 h [IQR: 3.0–16.0]) compared to the standard therapy (27.1 h [IQR: 20.3–48.0]; p = 0.002) [46]. In contrast, a phase 3 RCT of 121 patients and a smaller RCT of 30 patients reported no difference in time to discharge or time to symptom resolution between icatibant and placebo treatment [47, 48]. Meta-analysis indicated that those treated with icatibant experienced a statistically nonsignificant reduction in time to symptom resolution, relative to placebo treatment (mean difference: −7.77 h, 95% CI: −25.18–9.63) [49]. Further investigation is required before establishing the effectiveness of icatibant for drug-induced angioedema in the ED.
Two phase 2 RCTs examined the effectiveness of ecallantide for ACEi-induced angioedema in the ED [50, 51]. The primary endpoint was defined as the proportion of patients discharged within a prespecified time after treatment. In one study, with 4 h as the target time to discharge, 5/24 (21%) patients who received placebo met the endpoint, compared to 8/26 (31%) patients who received ecallantide [50]. In the study with 6 h as the discharge time, 13/18 (72%), 17/20 (85%), 17/19 (89%) and 17/19 (89%) patients receiving placebo, 10, 20 and 60 mg ecallantide, respectively, met the endpoint [51]. None of the differences in discharge time reached statistical significance in these two small studies.
Finally, in a retrospective case series of seven patients with presumed ACEi-induced angioedema refractory to standard treatment, patients were treated with FFP [52]. Symptoms improved in all of these cases, suggesting that FFP may be another effective therapy for drug-induced angioedema.
Limitations
The studies in this systematic review are small and mostly case series or individual case reports (Table 3). These studies also predominately include drug-induced attacks; not all forms of bradykinin-induced angioedema are represented. Despite these limitations, the literature reviewed here suggests approved HAE therapies may be effective for emergency treatment of various forms of bradykinin-induced angioedema. Awareness of bradykinin-induced angioedema and the therapeutic options for treating it will improve outcomes in the ED.
Conclusions
Angioedema, when affecting the upper airways, is a challenge for ED physicians because its two primary forms, histamine or bradykinin induced, cannot be readily distinguished on clinical grounds. Histamine-induced angioedema has a faster onset and often presents with urticaria, whilst bradykinin-induced angioedema is slower in onset, with greater incidence of abdominal symptoms. Initial evaluation should focus on airway management and treatment with epinephrine, antihistamine and systemic steroids according to anaphylactic protocols, except for known HAE patients and individuals with a history of drug-induced angioedema. When standard treatment is not effective, assuming proper treatment dosing and beta-adrenergic blockade have been addressed, bradykinin-induced angioedema should be considered and treated accordingly.
Although current approved therapies are indicated for HAE types I and II, Canadian HAE guidelines also recommend their use in patients with normal C1-INH [27]. It is tempting to speculate that the same can be applied to other forms of bradykinin-induced angioedema encountered in the ED. Even though more studies are required to establish this idea, these HAE therapies deserve consideration in emergency situations when standard therapies have failed.
Availability of data and materials
Not applicable.
Abbreviations
- ACE:
-
Angiotensin-converting enzyme
- C1-INH:
-
C1 esterase inhibitor
- ED:
-
Emergency department
- FDA:
-
Food and Drug Administration
- FcεRI:
-
High-affinity IgE receptors
- FFP:
-
Fresh frozen plasma
- HAE:
-
Hereditary angioedema
- HMWK:
-
High-molecular-weight kininogen
- IgE:
-
Immunoglobin E
- MHC:
-
Major histocompatibility
- Th:
-
T-helper
References
Bernstein JA, Cremonesi P, Hoffmann TK, Hollingsworth J. Angioedema in the emergency department: a practical guide to differential diagnosis and management. Int J Emerg Med. 2017;10(1):15.
Bernstein JA, Moellman J. Emerging concepts in the diagnosis and treatment of patients with undifferentiated angioedema. Int J Emerg Med. 2012;5(1):39.
Jaiganesh T, Wiese M, Hollingsworth J, Hughan C, Kamara M, Wood P, et al. Acute angioedema: recognition and management in the emergency department. Eur J Emerg Med. 2013;20(1):10–7.
Long BJ, Koyfman A, Gottlieb M. Evaluation and management of angioedema in the emergency department. West J Emerg Med. 2019;20(4):587–600.
Moellman JJ, Bernstein JA, Lindsell C. A consensus parameter for the evaluation and management of angioedema in the emergency department. Acad Emerg Med. 2014;21(4):469–84.
Burton OT, Oettgen HC. Beyond immediate hypersensitivity: Evolving roles for IgE antibodies in immune homeostasis and allergic diseases. Immunol Rev. 2011;242(1):128–43.
Gould HJ, Sutton BJ. IgE in allergy and asthma today. Nat Rev Immunol. 2008;8(3):205–17.
Kaplan AP, Joseph K, Silverberg M. Pathways for bradykinin formation and inflammatory disease. J Allergy Clin Immunol. 2002;109(2):195–209.
Busse PJ, Christiansen SC. Hereditary angioedema. N Engl J Med. 2020;382(12):1136–48.
Campbell DJ. Neprilysin inhibitors and bradykinin. Front Med (Lausanne). 2018;5:257.
Tang AW. A practical guide to anaphylaxis. Am Fam Physician. 2003;68:1325–32.
Cocchio C, Marzella N. Cinryze, a human plasma-derived C1 esterase inhibitor for prophylaxis of hereditary angioedema. PT. 2009;34(6):293–328.
Craig TJ, Levy RJ, Wasserman RL, Bewtra AK, Hurewitz D, Obtulowicz K, et al. Efficacy of human C1 esterase inhibitor concentrate compared with placebo in acute hereditary angioedema attacks. J Allergy Clin Immunol. 2009;124(4):801–8.
Cruz MP, Conestat alfa (Ruconest). First recombinant C1 esterase inhibitor for the treatmet of acute attacks in patients with hereditary angioedema. PT. 2015;40(2):PMC4315111.
Berinert. Prescribing Information. CSL Behring. 2021.
Cinryze. Prescribing information. U.S.A., Inc: Takeda Pharmaceuticals; 2021.
Ruconest. Prescribing information: Pharming Healthcare Inc; 2020.
Schneider L, Lumry W, Vegh A, Williams AH, Schmalbach T. Critical role of kallikrein in hereditary angioedema pathogenesis: a clinical trial of ecallantide, a novel kallikrein inhibitor. J Allergy Clin Immunol. 2007;120(2):416–22.
Farkas H, Reshef A, Aberer W, Caballero T, McCarthy L, Hao J, et al. Treatment effect and safety of Icatibant in pediatric patients with hereditary angioedema. J Allergy Clin Immunol Pract. 2017;5(6):1671–8.
Kalbitor. Prescribing information: Dyaz Corp; 2020.
Firazyr. Prescribing information. Takeda Pharmaceuticals America, Inc; 2020.
Berinert. Product monograph. Canada: CSL Behring; 2020.
Firazyr. Product monograph: Takeda Canada Inc; 2020.
Cinryze. Product monograph: Takeda Canada Inc; 2021.
Prematta M, Gibbs JG, Prat EL, Stoughton TR, Craig JC. Fresh frozen plasma for the treatment of hereditary angioedema. Ann Allergy Asthma Immunol. 2007;98(4):383–8.
Gupta A, Bigham M, Blood components. In: Clarke G, Chargé S, editors. Clinical guide to transfusion. Ottawa: Canadian Blood Services; 2021.
Betschel S, Badiou J, Binkley K, Borici-Mazi R, Hebert J, Kanani A, et al. The international/Canadian hereditary angioedema guideline. Allergy Asthma Clin Immunol. 2019;15:72.
Haegarda. Prescribing information: CSL Behring; 2020.
Takhzyro. Prescribing information: Dyaz Corp; 2018.
Bork K, Barnstedt SE. Treatment of 193 episodes of laryngeal edema with C1 inhibitor concentrate in patients with hereditary angioedema. Arch Intern Med. 2001;161:714–8.
Craig TJ, Wasserman RL, Levy RJ, Bewtra AK, Schneider L, Packer F, et al. Prospective study of rapid relief provided by C1 esterase inhibitor in emergency treatment of acute laryngeal attacks in hereditary angioedema. J Clin Immunol. 2010;30(6):823–9.
Gurmen ES, Dogan S, Sert E, Dikmetas C, Hussein S. Effect of C1 esterase inhibitor in hereditary angioedema treatment. Am J Emerg Med. 2017;35(6) 942:e5–6.
Yigit M, Sogut O, Lisar H, Yigit E. Usefulness of C1 esterase inhibitor protein concentrate in the management of hereditary angioedema of oropharyngeal tissue. Niger J Clin Pract. 2018;21(4):531–3.
Wentzel N, Panieri A, Ayazi M, Ntshalintshali SD, Pourpak Z, Hawarden D, et al. Fresh frozen plasma for on-demand hereditary angioedema treatment in South Africa and Iran. World Allergy Organ J. 2019;12(9):100049.
Pekdemir M, Ersel M, Aksay E, Yanturali S, Akturk A, Kiyan S. Effective treatment of hereditary angioedema with fresh frozen plama in a emergency department. J Emerg Med. 2007;33(2):137–9.
Erickson DL, Coop CA. Angiotensin-converting enzyme inhibitor-associated angioedema treated with C1-esterase inhibitor: a case report and review of the literature. Allergy Rhinol (Providence). 2016;7(3):168–71.
Greve J, Bas M, Hoffmann TK, Schuler PJ, Weller P, Kojda G, et al. Effect of C1-esterase-inhibitor in angiotensin-converting enzyme inhibitor-induced angioedema. Laryngoscope. 2015;125(6):e198–202.
Leibfried M, Kovary A. C1 esterase inhibitor (Berinert) for ACE inhibitor-induced angioedema: two case reports. J Pharm Pract. 2017;30(6):668–71.
Rasmussen ER, Bygum A. ACE-inhibitor induced angio-oedema treated with complement C1-inhibitor concentrate. BMJ Case Rep. 2013;2013:bcr2013200652.
Bartal C, Zeldetz V, Stavi V, Barski L. The role of icatibant-the B2 bradykinin receptor antagonist-in life-threatening laryngeal angioedema in the ED. Am J Emerg Med. 2015;33(3):479.e1–3.
Bas M, Greve J, Stelter K, Bier H, Stark T, Hoffmann TK, et al. Therapeutic efficacy of icatibant in angioedema induced by angiotensin-converting enzyme inhibitors: a case series. Ann Emerg Med. 2010;56(3):278–82.
Bova M, Guilarte M, Sala-Cunill A, Borrelli P, Rizzelli GM, Zanichelli A. Treatment of ACEI-related angioedema with icatibant: a case series. Intern Emerg Med. 2015;10(3):345–50.
Crooks NH, Patel J, Diwakar L, Smith FG. Icatibant in the treatment of angiotensin-converting enzyme inhibitor-induced angioedema. Case Rep. Crit Care. 2014;2014(17):864815.
Fok JS, Katelaris CH, Brown AF, Smith WB. Icatibant in angiotensin-converting enzyme (ACE) inhibitor-associated angioedema. Intern Med J. 2015;45(8):821–7.
Javaud N, Achamlal J, Reuter PG, Lapostolle F, Lekouara A, Youssef M, et al. Angioedema related to angiotensin-converting enzyme inhibitors: attack severity, treatment, and hospital admission in a prospective multicenter study. Medicine (Baltimore). 2015;94(45):e1939.
Baş M, Greve J, Stelter K, Havel M, Strassen U, Rotter N, et al. A randomized trial of icatibant in ACE-inhibitor-induced angioedema. N Engl J Med. 2015;372(5):418–25.
Sinert R, Levy P, Bernstein JA, Body R, Sivilotti MLA, Moellman J, et al. Randomized trial of icatibant for angiotensin-converting enzyme inhibitor-induced upper airway angioedema. J Allergy Clin Immunol Pract. 2017;5(5):1402–9.
Straka BT, Ramirez CE, Byrd JB, Stone E, Woodard-Grice A, Nian H, et al. Effect of bradykinin receptor antagonism on ACE inhibitor-associated angioedema. J Allergy Clin Immunol. 2017;140(1):242–8.
Jeon J, Lee YJ, Lee SY. Effect of icatibant on angiotensin-converting enzyme inhibitor-induced angioedema: a meta-analysis of randomized controlled trials. J Clin Pharm Ther. 2019;44(5):685–92.
Bernstein JA, Moellman JJ, Collins SP, Hart KW, Lindsell CJ. Effectiveness of ecallantide in treating angiotensin-converting enzyme inhibitor-induced angioedema in the emergency department. Ann Allergy Asthma Immunol. 2015;114(3):245–9.
Lewis LM, Graffeo C, Crosley P, Klausner HA, Clark CL, Frank A, et al. Ecallantide for the acute treatment of angiotensin-converting enzyme inhibitor-induced angioedema: a multicenter, randomized, controlled trial. Ann Emerg Med. 2015;65(2):204–13.
Hassen GW, Kalantari H, Parraga M, Chirurgi R, Meletiche C, Chan C, et al. Fresh frozen plasma for progressive and refractory angiotensin-converting enzyme inhibitor-induced angioedema. J Emerg Med. 2013;44(4):764–72.
Acknowledgements
Writing and editorial assistance was provided by Lisa Shao, MSc, and John Ashkenas, PhD of imc North America (Toronto, ON), supported by CSL Behring.
Funding
This project was investigator-initiated and investigator-driven. Support by Takeda for investigator meetings is gratefully acknowledged. Thanks also to CSL Behring for supporting the writing and editing of this manuscript.
Author information
Authors and Affiliations
Contributions
All of the authors contributed to the conception of the work and interpretation of the data. All of the authors drafted the manuscript, revised it critically for important intellectual content, gave final approval of the version to be published and agreed to be accountable for all aspects of the work.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
Jacques Hébert reports personal fees outside the submitted work for advisory boards and teaching from Takeda and CSL Behring. Hugo Chapdelaine declares grants outside the submitted work from Takeda, CSL Behring, Pharvaris, Dyax, Green Cross, Sanofi, Merck and Novartis. He also reports personal fees outside the submitted work from CSL Behring, Takeda and Sobi. He is also an associate review editor with Frontiers in Immunology. Benoit Laramée declares participating in advisory committees or presentations from ALK, Takeda, CSL Behring, Novartis and Pedia-Pharm. Rémi Gagnon declares being a principal investigator on HAE trials funded by BioCryst, Takeda, CSL Behring and Pharvaris. No other competing interests were declared.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Hébert, J., Boursiquot, JN., Chapdelaine, H. et al. Bradykinin-induced angioedema in the emergency department. Int J Emerg Med 15, 15 (2022). https://doi.org/10.1186/s12245-022-00408-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12245-022-00408-6